Can an Autistic Be Too Old to Get a New Special Interest?
Autistic and wondering if getting older means a “burning out” of your capacity for new special interests? […]

Autistic and wondering if getting older means a “burning out” of your capacity for new special interests? […]
Truly inspirational women don’t obsessively preach that influencers post the best photo and delete the rest. Enough of this virtue signaling already. […]
When’s the worst time in adulthood to pile on the pounds? […]
It’s not a myth: When you eat can contribute to your weight loss goals. It’s no longer just about portions, sugar and macronutrients. Timing is important. […]
I was watching a true crime documentary and the narrator said the victim’s young son “had a mild form of neurodivergence” and had to go to a special school. Hey, just say AUTISM! [...]
It’s common for a psychologist to want to interview the parents of an adult seeking an autism assessment. But this can backfire. […]
Videos of nonspeaking autistic people using rapid prompting method usually show a fixed, uniform tapping with their index finger – as though tapping to a music beat. […]
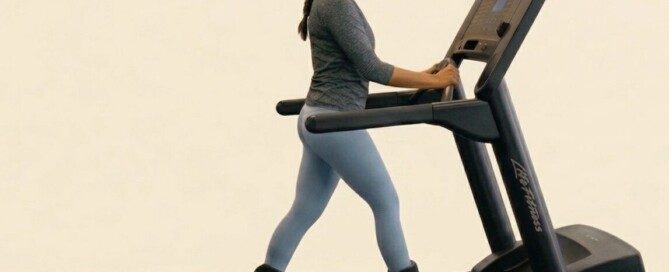
I saw a woman wearing ankle weights as she walked on an inclined treadmill, but she was holding on. […]
Chronic inflammation doesn’t always announce itself. In many cases it develops quietly in the background like malware, with little pain or obvious warning signs. […]
Why is the music so loud at Starbucks? It’s a coffeehouse, not a nightclub! […]
Many autistic people eat the same foods day after day. But this approach to food intake has been shown by research to aid in weight loss. […]
A large study suggests you don’t need long workouts to improve your health. […]
If you’re suffering from osteoarthritis knee pain, this doesn’t mean that exercise can’t improve your situation. […]
Did Woody Brown write “Upward Bound” or did mom Mary pen this novel? Why would this mom falsely claim her nonverbal, severely autistic son wrote it? […]
How did Mary Brown convince college professors to give her nonverbal son Woody two degrees when there’s video proof he can’t spell a single word? […]
Naïve people who defend Woody Brown’s tapping at a letter board without looking have compared this to touch typing. […]
If you have severe upper back pain, there’s one test you’d better make sure the ER gives you; otherwise you may end up dead from multi-organ failure. […]
Mom is promoting her nonspeaking autistic son’s novel. The talk show made the error of an up-close shot of the letter board as Woody “spelled” – gibberish. […]
Having your older autistic child in a wagon when you’re out in the community may prevent elopement, but over time, muscle atrophy will occur. […]
Woody Brown doesn’t look at the letter board as he allegedly spells. Mom explains this away by saying he needs to look elsewhere to maintain focus. […]
Your chances of dying early are greatly increased if you have both excess belly fat and untrained flaccid muscles. […]
Lifting weights doesn't make you a lunkhead; research says it makes the brain younger and improves cognition. Who wouldn't want a younger sharper brain? But wait... This doesn't mean you need to bulk up or [...]
A slimmer waistline is more about heart health than beauty standards. […]
Are you a senior and looking for a sustainable way to exercise but find the idea of walking, jogging and yoga boring or off-putting? […]
Even small amounts of resistance training can build strength, increase muscle size, improve power and support overall physical function. […]
Is there a sneaky question that if you asked someone who’s autistic, their answer would reveal their autism? I don’t mean “Are you autistic?” […]
A pulmonary embolism can strike even the fittest of people and be caused by a long airline flight when someone hardly moves their legs. […]
Men get varicose veins too, but even if a man doesn’t care about looks, he needs to worry about possible medical complications of these abnormal vein formations. […]
“Overdo” things recently and aggravate your chronic low back pain? Do you think the solution is to live the rest of your life “taking it easy”? […]
Inactivity will quicken disability if you have knee osteoarthritis, while exercise will greatly delay the need for a total knee replacement. […]
The current gold standard for sleep apnea treatment is a CPAP machine, which is intolerable by many. Wouldn’t it be great if a pill could replace a CPAP? […]
Sleeping and heart health are strongly linked, and more and more research is showing this. […]
Worrying about getting old might actually quicken the aging process, especially for women. […]
It’s quite possible that the highest functioning of Autistics have it the roughest. […]
There’s something oddly insulting about the claim that whenever a woman wants to lose weight it’s because she’s been brainwashed by society. […]
The shaming of women who want weight loss, especially via GLP-1 drugs, needs to stop. Easily triggered influencers are the primary culprits. This includes influencers who’ve never used a GLP-1 or who’ve never even been [...]
Do you “look” too typical for your autism diagnosis to be believed and thus wish you “looked autistic” so people would stop thinking you’re incompetent, lazy, rude and other negative things? […]
Just get a late autism diagnosis but question it because you don’t stim? Maybe you really DO stim but don’t realize just how much. Here’s how to figure all of this out. […]
Shouldn’t a “dad bod” be the buff one rather than the soft paunchy one? After all, men who do more screen time than kid time are more likely to have that dad bod. [...]
Have you discovered that when walking on your home treadmill, one of your feet “drags,” that is, you can tell it’s making more contact with the belt than your other foot is? […]
MOLES AND MELANOMA


































.





























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}